 BASICS
BASICS
- Fructose and Polyunsaturated Oils create a susceptible organ.
- The incidence of Cancer is increasing.
- The incidence of Childhood Cancer is increasing.
- The development of ‘Western’ Cancers mimics the introduction of ‘Western’ food in to Papua New Guinea, the Inuit Eskimos and Vanuatu.
- The social and economic cost of the Burden of Disease from Cancer alone is not sustainable in any country.
- Nutritional ketosis should sensitise cancers to the treatments of chemotherapy and radiotherapy and protect the surrounding cells from the side effects of treatment.
_________________
Nutrition and Cancer – Time to Rethink
The video to allow you to take back some control in cancer management. September 7 2015.
_________________
IDEAS
Cancer Epidemic
The combination of Fructose and Polyunsaturated Oils create a susceptible organ on which a trigger can act and that susceptibility allows the growth of abnormal cells.
The medical community is spending the vast amount of research resources looking at triggers for Cancer development and on the treatment. It is the ‘tail wagging the dog’.
We have not spent the time or effort looking at the vulnerable person – and why that is probably more important than the trigger.
My overall impression is that our modern cancer epidemic is probably related in the proportions of 60% fructose, 30% polyunsaturated oils and 10% for all of the other things which we consider to be factors.
As to these numbers being exact it is clearly an approximation but until we address the primary issue then we are going nowhere on this vast issue.
Research money needs to be considered for this concept.
______________________________
Future of Cancer – Time to Rethink?
Gary Fettke Cape Town talk Feb 2015
“Could we have been travelling down the wrong road of cancer treatment for 90 years? This opens up a whole new way of managing cancer, based on a nutritional approach that is cheaper and doesn’t have the bad side effects of conventional treatment.
Cancer rates are rising worldwide. We never used to see cancers in traditional societies, such as the Inuit and the people of New Guinea, but now we do. Estimates are that there will be a 70% increase in cancers over the next 20 years especially in developing nations, and there is already a 3% increase in children’s cancers per annum. One in two men and one in three women will develop cancer.
There is an increasing incidence of worldwide cancer and poorer prognosis.
The genetic model of cancer doesn’t make sense. It raises the question: is cancer a problem of chromosomal damage as we’ve been taught? But what if the chromosomal damage is just a cancer marker, not the cause. What if the model is wrong, if we are doing things the wrong way when treating cancer? If we have been going down the wrong road for 90 years?”
The summary of the talk is at http://www.nofructose.com/2015/02/26/future-of-cancer-time-to-rethink/
_______________________________
Cancer and Nutrition – Time to Rethink
Cancer – What happens if you or someone you love is given that diagnosis?
What are you going to do? Two options.
1. Go to each doctor visit and each test and lurch from one result to another in an uncontrolled manner. Scary but that’s what happens to most people. I have been there.
2. Do something yourself and take back some control. Know that you are doing what you can to weaken the cancer and strengthen the cells around the cancer.
I believe that nutritional ketosis puts most cancers on the back foot. It is a great adjunctive treatment.
It is not about replacing traditional treatments of surgery, radiotherapy and chemotherapy.
I have had cancer. I am in nutritional ketosis. I want to make it as hard as possible for it to come back.
That’s what I am doing. Want to learn more?
Here is my recent Brisbane talk at https://youtu.be/qa5Bcm8T9nU
More at http://www.nofructose.com/health-issues/cancer/
https://www.facebook.com/permalink.php?story_fbid=953004368127348&id=393958287365295
16 January 2016
____________________________
2015 LCHF World Summit Lecture Series
“The most significant medical event since the first human heart transplant.”
Here it is. The cancer lecture is now available online. I was a student and a teacher in the one event. What a privilege it was to be part of this event. Watch these and you will learn – guaranteed.

_________________________________
Theoretical Cancer Model
There are three phases to the development of a cancer with relationship to my theory. The same applies to most other disease.
Phase 1
The first is that if to create low grade inflammation. The cell in an organ then undergoes what is called metaplasia, just like you develop a callus on the bottom of your foot when running barefoot over time. That chronic irritation creates a change in cells. If irritation continues over a longer period of time then those cells can start developing abnormalities and some of them may in fact turn into cancer cells (dysplasia and in to anaplasia).
Phase 2
Those cells then have the ability to divide and if they are in the right inflamed and vascular environment they can potentially grow.
Phase 3
The third aspect is that the body has natural clearing mechanisms within it for taking away abnormal cells and material. There are white cells that are responsible for this activity. Under a Fructose high environment, they appear to have poorer function and motility. This means you have a relatively immunosuppressed system for clearing up any abnormal cells that are developing in the body.
The combination of these three entities with increasing abnormal cells, growing in an inflamed environment and not being able to be cleared away falls well within a model for creating a cancer.
I clearly feel this requires further research and maybe that is the next step we are heading towards.
Childhood Cancer
If the mother takes in a diet with Polyunsaturates Oils then that it will make its way into the embryo, foetus and then breast milk.
The potential damage for the child from polyunsaturated oil consumption may therefore be happening in the womb (in utero), continue on with breast milk and then be compounded as the child is weaned off breast milk.
Could this be a model for the rising incidence of childhood Cancer, allergy and disease?
_________________________
 Biochemistry of Religion
Biochemistry of Religion
Just for once have we considered the common feature of all religions. They have all respected the one thing for thousands of years. What is it that has brought around clarity of thought, health and well-being. It’s all in the ‘Biochemistry of Religion’.
Here is an excerpt from one of my talks.
___________________________________
Starving Cancer Blog
Facebook Blog March 3 2013
Trials are underway looking at decreasing calories in patients with cancer rather than increasing them. It sort of make sense to starve the most rapid turnover cells rather than feed them.
It is history repeating itself from mice experiments a 100 years ago and tags on to work originally out of South America where it was noticed that patients on Metformin (a cheap anti diabetes drug) had a slower progression of their cancers. Metformin is now mainstream management.
There is a long way to go on this topic but the epidemiology of disease is driving the science.
Know someone affected by Cancer?
Facebook Blog April 4 2013
I do. Just coming up to my 13 year anniversary of my own Cancer. Two lots of Surgery, and Intensive Care each time, followed by radiotherapy and then chemotherapy on and off for years. Not much fun but I am still here.
I now understand why I had Cancer at age 38. I understand why my mother died at the ‘old’ age of 53 when I was a teenager. I understand why the rate of Cancer in all society is escalating and why the rate of Childhood Cancer is going up 3% per annum.
At least I have a theoretical model of why.
The combination of Fructose and Polyunsaturated Oils create a susceptible organ on which a trigger can act and that susceptibility allows the growth of abnormal cells.
The medical community is spending the vast amount of research resources looking at triggers for Cancer development and on the treatment. It is the ‘tail wagging the dog’.
We have not spent the time or effort looking at the vulnerable person – at you – and why that is probably more important than the trigger.
_____________________________
Can we Eat to Starve Cancer?
“What we eat is our chemotherapy three times a day.”
Facebook blog 24 September 2013
Angiogenesis is the ability for blood vessels to grow and every cancer needs a blood supply and fuel.
If we can stop inappropriate blood vessel growth then we can prevent, slow and cure cancer. Almost too good to be true but it is one of the frontiers of Cancer therapy.
I believe that our diet and particularly the combination of Fructose and Polyunsaturated Oils combine to create inflammation in every blood vessel and therefore in every organ. That creates a susceptible organ which is prone to damage from a variety of genetic and environmental factors.
When you are rundown then your immune system is down too. Imagine your diet being responsible for you being chronically inflamed every day of your life and even as an embryo – welcome to modern disease.
Add in the insulin spikes associated with high carbohydrate loads and there is more stimulation to growth of tumour cells.
Dr William Li of the Angiogenesis Foundation explores the Angiogenesis topic in this TED talk from 2010.
http://www.youtube.com/watch?v=B9bDZ5-zPtY
His concepts fit neatly with my ideas of the metabolic model of cancer and particularly the inflammatory aspect.
Anti-inflammatories help in cancer management and the best anti-inflammatory management is in our diet.
He talks about what we can do for ourselves and that we should be eating local and sustainable food that is anti-angiogenetic. And he gives the thumbs up to red wine. I think the tomatoes are the answer and not the sauce though.
“What we eat is our chemotherapy three times a day”
If you have time, watch the short animation at the end of the TED talk. I posted it yesterday and many of you have seen it already. The vast majority of us are just looking out of our windows just watching the health disaster unfold. Brilliant.
________________________
Starve Cancer Now
 ‘Is there a way to exploit the metabolic quirk of cancer?’
‘Is there a way to exploit the metabolic quirk of cancer?’
Peter Attia has summarised a topic dear to my heart. It is how I have stumbled and tumbled down the No Fructose pathway.
Glucose is selectively taken up by many cancer cells. By starving these cells from glucose and insulin spikes in the bloodstream then it makes sense that it may be a path to managing and at least preventing cancer.
It is why I have drifted from a No Fructose diet to being into the very low carbohydrate and higher fat diet. I am ‘starving’ the troublesome cells in my body.
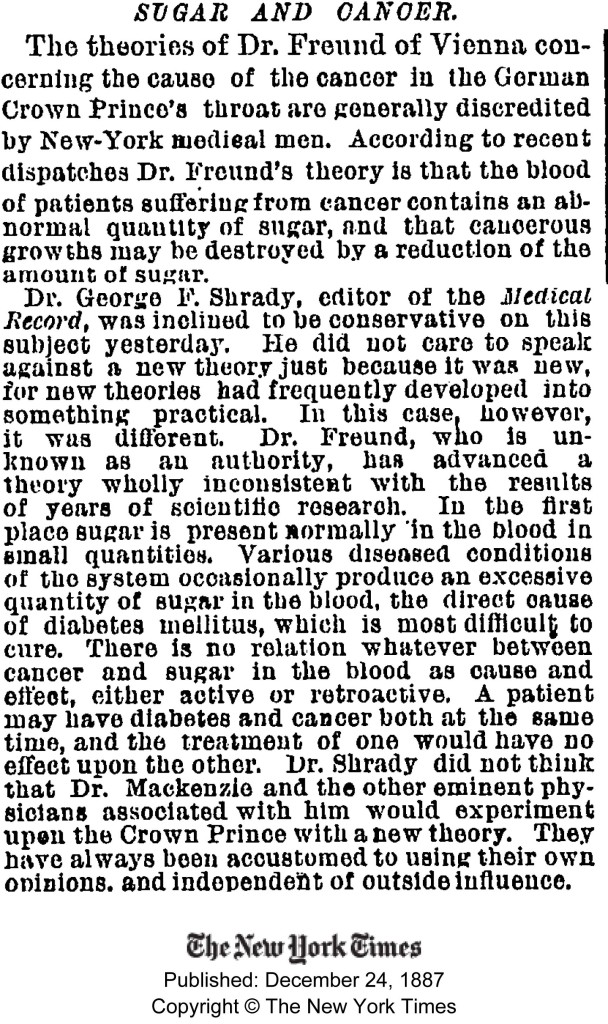
Do yourself a favour and read his blog but also enlarging the photo and reading this 1887 article in the New York Times.
“Dr Freunds theory is that the blood of patients suffering from cancer contains an abnormal quantity of sugar, and that cancerous growths may be destroyed by a reduction of the amount of sugar.”
We are reinventing the wheel and about time!
http://eatingacademy.com/nutrition/way-exploit-metabolic-quirk-cancer
MORE INFORMATION
There has been a 27 percent increase in the worldwide Burden of Cancer in the last 10 years which shows the situation is clearly out of control. This is a major unsustainable economic burden on society, and particularly those in developing nations.
___________________
Cancer and Obesity
http://feinmantheother.com/2012/09/03/suddenly-last-summer-the-triumph-of-carbohydrate-restriction/
___________________
Calorie restriction in a mouse model
https://dl.dropboxusercontent.com/u/37202414/Sabatini_restriction%29Nature_2009.pdf
________________
Read about the Damage Process
The NoFructose Handout Starter Sheet is your take away summary of this web site. Read it at the NoFructose Starter Sheet area of this web site or download it.
Please add information by going to Contribute to NoFructose.com
ARTICLES
Lancet sustainable development1-s2.0-S0140673613601385-main
Lancet 2 2013 editorial stop cancer now1-s2.0-S0140673613600598-main
This Lancet editorial is related to the increasing incidence of cancer across the world. There has been a 27 percent increase in cancer in the last 10 years which shows the situation is clearly getting out of control. This is a major economic burden on society, and particularly those developing nations.
Lancet Cancer BOD 1-s2.0-S0140673613601762-main
Lancet stop cancer now 1-s2.0-S0140673613600604-main
Obesity and Cancer Risk
Body-mass index and cancer mortality in the Asia-Pacific Cohort Studies Collaboration: pooled analyses of 424,519 participants.
Lancet Oncol. 2010 Aug;11(8):741-52. doi: 10.1016/S1470-2045(10)70141-8. Epub 2010 Jun 30.
BACKGROUND: Excess bodyweight is an established risk factor for several types of cancer, but there are sparse data from Asian populations, where the proportion of overweight and obese individuals is increasing rapidly and adiposity can be substantially greater for the same body-mass index (BMI) compared with people from Western populations.
METHODS: We examined associations of adult BMI with cancer mortality (overall and for 20 cancer sites) in geographic populations from Asia and from Australia and New Zealand (ANZ), within the Asia-Pacific Cohort Studies Collaboration, by use of Cox regression analysis. Pooled data from 39 cohorts (recruitment 1961-99, median follow-up 4 years) were analysed for 424,519 participants (77% Asian; 41% female; mean recruitment age 48 years) with individual data on BMI.
FINDINGS: After excluding those with follow-up of less than 3 years, 4872 cancer deaths occurred in 401,215 participants. Hazard ratios for cancer sites with increased mortality risk in obese (BMI > or = 30 kg/m(2)) compared with normal weight participants (BMI 18.5-24.9 kg/m(2)) were: 1.21 (95% CI 1.09-1.36) for all-cause cancer (excluding lung and upper aerodigestive tract), 1.50 (1.13-1.99) for colon, 1.68 (1.06-2.67) for rectum, 1.63 (1.13-2.35) for breast in women 60 years or older, 2.62 (1.57-4.37) for ovary, 4.21 (1.89-9.39) for cervix, 1.45 (0.97-2.19) for prostate, and 1.66 (1.03-2.68) for leukaemia (all after left censoring at 3 years). The increased risk associated with a 5-unit increase in BMI for those with BMI of 18.5 kg/m(2) or higher was 1.09 (95% CI 1.04-1.14) for all cancers (excluding lung and upper aerodigestive tract). There was little evidence of regional differences in relative risk of cancer with higher BMI, apart from cancers of the oropharynx and larynx, where the association was inverse in ANZ and absent in Asia.
INTERPRETATION: Overweight and obese individuals in populations across the Asia-Pacific region have a significantly increased risk of mortality from cancer. Strategies to prevent individuals from becoming overweight and obese in Asia are needed to reduce the burden of cancer that is expected if the obesity epidemic continues.
The link between diet and cancer.
A lot hinges around the role of insulin on stimulating factors involved in cellular division and metabolism.
A diet high in fructose and refined fibreless carbohydrate just keeps hammering away at the pancreas, giving us insulin spikes and a chronic stimulation of the system, ultimately responding in an insulin resistance.
This review article by Dr Elio Riboli notes the increased risk of late onset breast cancer, colon, rectum, endometrial, oesophageal and kidney cancers with obesity. He touches on the association between high sugar and carbohydrate load in the article.
I agree with him on the concept of where we were with the links of tobacco and disease were known for a long time but action took longer.
http://www.biomedcentral.com/1741-7007/12/9
____________________
New insights into the health effects of dietary saturated and omega-6 and omega-3 polyunsaturated fatty acids
2012
 1 and
1 and Cardiovascular diseases and cancers are leading causes of morbidity and mortality. Reducing dietary saturated fat and replacing it with polyunsaturated fat is still the main dietary strategy to prevent cardiovascular diseases, although major flaws have been reported in the analyses supporting this approach. Recent studies introducing the concept of myocardial preconditioning have opened new avenues to understand the complex interplay between the various lipids and the risk of cardiovascular diseases. The optimal dietary fat profile includes a low intake of both saturated and omega-6 fatty acids and a moderate intake of omega-3 fatty acids. This profile is quite similar to the Mediterranean diet. On the other hand, recent studies have found a positive association between omega-6 and breast cancer risk. In contrast, omega-3 fatty acids do have anticancer properties. It has been shown that certain (Mediterranean) polyphenols significantly increase the endogenous synthesis of omega-3 whereas high intake of omega-6 decreases it. Finally, epidemiological studies suggest that a high omega-3 to omega-6 ratio may be the optimal strategy to decrease breast cancer risk. Thus, the present high intake of omega-6 in many countries is definitely not the optimal strategy to prevent cardiovascular disease and cancers. A moderate intake of plant and marine omega-3 in the context of the traditional Mediterranean diet (low in saturated and omega-6 fatty acids but high in plant monounsaturated fat) appears to be the best approach to reduce the risk of both cardiovascular diseases and cancers, in particular breast cancer.
_____________
The Israeli Paradox’ – Following ‘Modern’ Fietary advice is associated with higher rates of cancer, cardiovascular disease and obesity.
Diet and disease–the Israeli paradox: possible dangers of a high omega-6 polyunsaturated fatty acid diet.
Israel has one of the highest dietary polyunsaturated/saturated fat ratios in the world; the consumption of omega-6 polyunsaturated fatty acids (PUFA) is about 8% higher than in the USA, and 10-12% higher than in most European countries. In fact, Israeli Jews may be regarded as a population-based dietary experiment of the effect of a high omega-6 PUFA diet, a diet that until recently was widely recommended. Despite such national habits, there is paradoxically a high prevalence of cardiovascular diseases, hypertension, non-insulin-dependent diabetes mellitus and obesity-all diseases that are associated with hyperinsulinemia (HI) and insulin resistance (IR), and grouped together as the insulin resistance syndrome or syndrome X. There is also an increased cancer incidence and mortality rate, especially in women, compared with western countries. Studies suggest that high omega-6 linoleic acid consumption might aggravate HI and IR, in addition to being a substrate for lipid peroxidation and free radical formation. Thus, rather than being beneficial, high omega-6 PUFA diets may have some long-term side effects, within the cluster of hyperinsulinemia, atherosclerosis and tumorigenesis.
____________________________
Women’s higher risk with N-6 PUFA vs. men’s relative advantage: an “N-6 gender nutrition paradox” hypothesis.
Abstract
The “Israeli Paradox” (1996) of low national health rankings despite adequate diet – attributed to high dietary n-6 polyunsaturated fatty acids (PUFA) – coincided with long-observed dichotomies between women’s worse international status vs. men’s advantage. This raised the possibility of a gender link to high n-6 risk potentially explaining both national phenomena. Israeli women’s disadvantage was shown by worse international rankings, i.e., life expectancy (LE)–11th vs. men’s 3rd-best/22 countries (2000), and 14th vs. 6th/34 (2010); and all-cause and all-cancer mortality–both 15th vs. 2nd-best/22 (2000), and 15th vs. 6th/22 and 12th vs. 2nd-best/22 (2010). Cancer mortality rates for breast were 21.8% above vs. prostate 30.4% below Eur-A (27 country) averages (2005). Gender gaps/ ratios were smaller than European Union-15 averages, i.e., for LE at birth by 34.4-26.4% (2000-2010), respectively, and at 65 years 45.9-35.3%; all-cause mortality by 43.3-33.4%, and all-cancer 65.2-58.7%. The Israeli diet was mostly close to guidelines, but n-6 intake (10-12% kcal) was much higher than recommended and traditional “Mediterranean diet” levels. Research showing females’ greater potential for conversion of PUFA to long-chain PUFA (LCPUFA) may suggest increased production of n-6 eicosanoids with known proinflammatory/oxidative/carcinogenic potential. An “Israeli N-6 Gender Nutrition Paradox” hypothesis is suggested here for the first time, associating women’s higher risk and lead in the national “paradox” with greater potential for n-6 conversion to pro-inflammatory/oxidative/carcinogenic eicosanoids compared to men. This may also exacerbate women’s risk associated with genetic predisposition (i.e., BRCA) and/or sociopolitical stress. Global abandonment of traditional diets/foods together with increasing n-6 consumption and western disease rates emphasize the importance of considering gender nutrition in epidemiology and preventive strategies.
____________________________
Women’s higher health risks in the obesogenic environment: a gender nutrition approach to metabolic dimorphism with predictive, preventive, and personalised medicine.
Women’s evolution for nurturing and fat accumulation, which historically yielded health and longevity advantages against scarcity, may now be counteracted by increasing risks in the obesogenic environment, recently shown by narrowing gender health gap. Women’s differential metabolism/disease risks, i.e. in fat accumulation/distribution, exemplified during puberty/adolescence, suggest gender dimorphism with obesity outcomes. Women’s higher body fat percentage than men, even with equal body mass index, may be a better risk predictor. Differential metabolic responses to weight-reduction diets, with women’s lower abdominal fat loss, better response to high-protein vs. high-carbohydrate diets, higher risks with sedentariness vs. exercise benefits, and tendency toward delayed manifestation of central obesity, metabolic syndrome, diabetes, cardiovascular disease, and certain cancers until menopause-but accelerated thereafter-suggest a need for differing metabolic and chronological perspectives for prevention/intervention. These perspectives, including women’s differential responses to lifestyle changes, strongly support further research with a gender nutrition emphasis within predictive, preventive, and personalized medicine.
____________________________
A high ratio of dietary n-6/n-3 polyunsaturated fatty acids is associated with increased risk of prostate cancer.
Abstract
Experimental studies suggest omega-3 (n-3) polyunsaturated fatty acids (PUFA) suppress and n-6 PUFA promote prostate tumor carcinogenesis. Epidemiologic evidence remains inconclusive. The objectives of this study were to examine the association between n-3 and n-6 PUFA and prostate cancer risk and determine if these associations differ by race or disease aggressiveness. We hypothesize that high intakes of n-3 and n-6 PUFA will be associated with lower and higher prostate cancer risk, respectively. A case-control study comprising 79 prostate cancer cases and 187 controls was conducted at the Durham VA Medical Center. Diet was assessed using a food frequency questionnaire. Logistic regression analyses were used to obtain odds ratios (ORs) and 95% confidence intervals (95% CI) for the associations between n-3 and n-6 PUFA intakes, the dietary ratio of n-6/n-3 fatty acids, and prostate cancer risk. Our results showed no significant associations between specific n-3 or n-6 PUFA intakes and prostate cancer risk. The highest dietary ratio of n-6/n-3 was significantly associated with elevated risk of high-grade (OR, 3.55; 95% CI, 1.18-10.69; P(trend) = 0.03), but not low-grade prostate cancer (OR, 0.95; 95% CI, 0.43-2.17). In race-specific analyses, an increasing dietary ratio of n-6/n-3 fatty acids correlated with higher prostate cancer risk among white men (P(trend) = 0.05), but not black men. In conclusion, our findings suggest that a high dietary ratio of n-6/n-3 fatty acids may increase the risk of overall prostate cancer among white men and possibly increase the risk of high-grade prostate cancer among all men.
____________________
Effect of n-3 and n-6 unsaturated fatty acids on prostate cancer (PC-3) and prostate epithelial (RWPE-1) cells in vitro.
Abstract
Prostate cancer (PCa) is one of the leading causes of death in the elderly men. Polyunsaturated fatty acids (PUFAs) regulate proliferation of cancer cells. In the present study, we evaluated the effect of various PUFAs on the proliferation and survival of human prostate cancer (PC-3) and human prostate epithelial (RWPE-1) cells in vitro.LA, GLA, AA, ALA, EPA and DHA (linoleic acid, gamma-linolenic acid, arachidonic acid, alpha-linolenic acid, eicosapentaenoic acid and docosahexaenoic acid respectively) when tested at 50, 100, 150, and 200 μM inhibited proliferation of RWPE-1 and PC-3 cells, except that lower concentrations of LA (25 μM) and GLA (5, 10 μM) promoted proliferation. Though all fatty acids tested produced changes in the production of interleukin-6 (IL-6), tumor necrosis factor-α (TNF-α), lipoxin A4 and free radical generation by RWPE-1 and PC-3 cells, there were significant differences in their ability to do so. As expected, supplementation of various n-3 and n-6 fatty acids to RWPE-1 and PC-3 cells enhanced the content of the added fatty acids and their long-chain metabolites in these cells. In contrast to previous results, we did not find any direct correlation between inhibition of cell proliferation induced by various fatty acids and free radical generation. These results suggest that polyunsaturated fatty acids suppress proliferation of normal and tumor cells by a variety of mechanisms that may partly depend on the type(s) of cell(s) being tested and the way these fatty acids are handled by the cells. Hence, it is suggested that more deeper and comprehensive studies are needed to understand the actions of fatty acids on the growth of normal and tumor cells.
_______________________