 BASICS
BASICS
The consumption of Sugar and Polyunsaturated Seed Oils combine in our diet to create inflammation in every blood vessel wall and in every tissue in every organ of the body. The inflammatory process makes everything susceptible to further damage and disease.
The NoFructose Handout Starter Sheet is your take away summary of this web site. Read it at the NoFructose Starter Sheet area of this web site or download it.
IDEAS
Reversing the consumption of Fructose and Polyunsaturated Seed Oils should reverse the inflammation in our bodies and allow the body to repair itself.
What is the fuss about Fructose and Polyunsaturated Fats?
The amount and frequency of Fructose and Polyunsaturated Fat consumption combine in our diet to create the ‘Perfect Storm’ of inflammation in every blood vessel wall in every organ of the body.
It just finally makes sense! Something has happened to our dietary intake in the last 100 years or so to account for the massive shifts in diseases modern society is experiencing.
My interpretation is that the combination creates a chronic inflammation in every organ of the body. This makes that part of the body then susceptible to a variety of other influences including genetics, the chemicals in our society, radiation and whatever the media throws at us on a week to week basis.
The chronic inflammation in the organs is predominantly related to the by-products of fructose and polyunsaturated fat metabolism.
The small LDL’s (The ‘Bad’ part of the ‘Bad LDL’ lipoproteins when you have your ‘cholesterol’ checked) produced by our metabolism of Fructose are the ‘Goldilocks’ size in that they are just the right size to get into the subintimal layer of every blood vessel. They then sit there and are oxidised (just like steel rusts). This creates inflammation in the vessels and the organs themselves.
The higher the proportion of polyunsaturated fats within those lipoproteins, the greater the intensity of the inflammation that occurs. If the LDL’s are full of saturated fats (animal fats) there is less oxidation and inflammation that then occurs.
Complicated but simple.
MORE INFORMATION
Damage Process
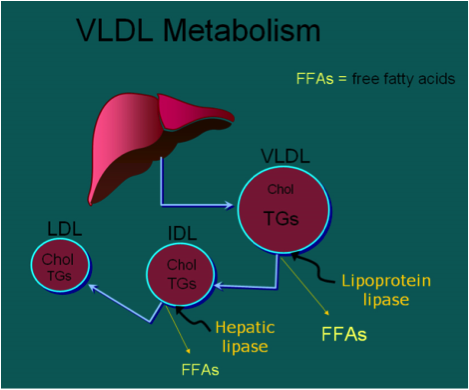
Fructose is metabolised in the liver into fatty acids, which are then transported as very low density lipoproteins (VLDLs) and are then converted into circulating intermediate density lipoproteins (IDLs) and then converted into low density lipoproteins (LDLs).
The LDLs are what I call the ‘Goldilocks’ size. Just the right size to sneak through the endothelial wall of every blood vessel and then sit in the subintimal layer between the endothelium and the smooth muscle of a blood vessel wall. This is one of my favourite diagrams for explaining the process.
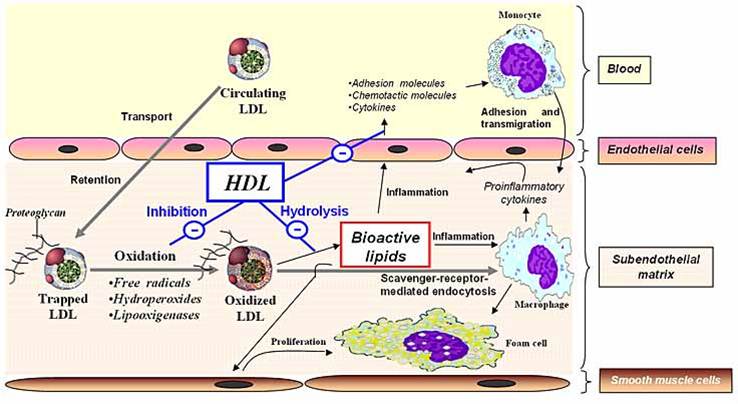
It is in this area that the trapped LDLs become oxidised and the inflammatory process then occurs creating a combination of macrophages and foam cells, ultimately leading to what we know as atherosclerotic plaque. The greater the percentage of polyunsaturated oils or fats within the trapped LDL, the greater the rate of oxidation and the greater the inflammation. If the LDL is full of saturated fat the oxidation process is obviously far less.
The above diagram shows high density lipoproteins (HDLs) which are high density lipoproteins trying to act as a clearing mechanism but with our current fructose load within the system is probably too late for the HDLs to do their clearing properly. 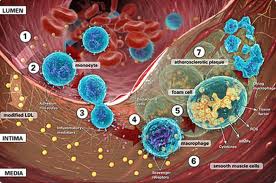
This diagram illustrates the small ‘yellow’ LDL particles, which are able to sneak through the endothelial wall in the subintimal layer. The large macrophages are the body’s immune response to that inflammation which then attempt to mop it up. The resultant effect is the development of foam cells which are the ones noted normally in atherosclerotic plaque.
The fats and oils in our body fall into a few categories. There are those that are saturated, those that are monounsaturated and those that are polyunsaturated.
If fat is made up of saturated molecules then it is fairly inflexible and solid at room temperature. Because of its inflexibility it doesn’t really have any weak spots which can be oxidised or ‘rusted’.
Saturated fats are predominantly found in animals, which are heated up to our normal body temperature of around 37 degrees Celsius. At room temperature they are generally solid like butter and lard.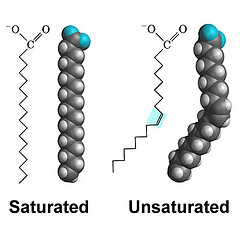
Monounsaturated fat has a single double bond in it to give it some flexibility and polyunsaturated fat has multiple double bonds within it to give it significant flexibility.
The polyunsaturated fats tend to come from plants where that flexibility allows them to be liquid at room and cold temperatures so that a plant can survive in cold areas. This allows for mobility of nutrients within the plant.
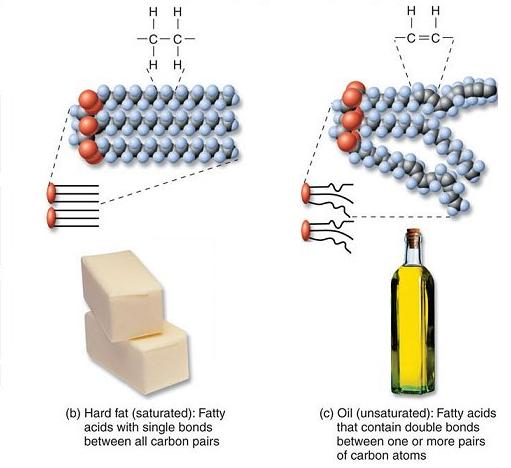
This diagram reflects the combination of saturated fats versus polyunsaturated fat. The saturated fats found in animal products such as butter and lard do not really have any side arms which allow flexibility and therefore do not really allow the potential for oxidation to occur. The polyunsaturated fats however have multiple side arms and provide ‘weak’ spots for oxidation to occur and subsequent inflammation to occur.
The best analogy I can give is that a piece of steel out in the weather in an untreated form rusts quite rapidly. A piece of stainless steel which does not have any weak spots or side arms for oxidation can stay out in the weather for a long period of time without the same issue.There is no real effective difference between that of saturated fats to polyunsaturated fats with this analogy.
As time progresses the proportion of polyunsaturated fats that come into our diet then make their way into the lipoproteins, which transport the fats around the body. The fats by themselves are not soluble in water, therefore they are transported with proteins to make up lipoprotein material. They then make their way into the arterial walls and into the tissues of the body.
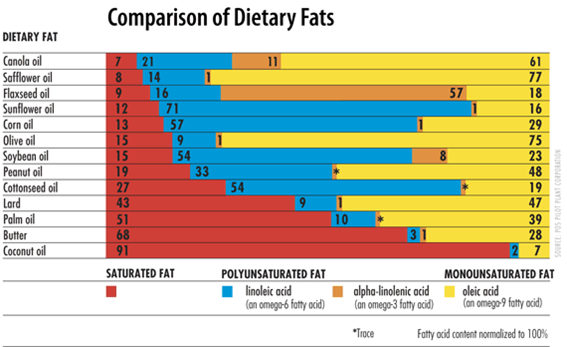
The main determinant of the proportion of Saturated, Monounsaturated and Polyunsaturated fats within our circulating lipoproteins and within tissue fat stores is the same as our diet. The western, modern diet has changed to a greater portion of Polyunsaturated fats over the last 50 to 100 years and this is reflected in the tissue accumulation of this component.
The greater the proportion of polyunsaturated fats within tissue the more likely for oxidation and inflammation to occur. The more saturated the proportion then the less oxidation occurs.
There has been an ongoing increase in the proportion of polyunsaturated fats found within subcutaneous fat tissue in the body as evidenced by the graph below out of the US body fat over the last 50 years.
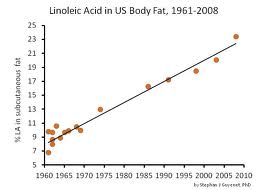
The net effect of a rising percentage of linoleic acid (major component of polyunsaturated oil) is that there is a far greater proportion of fat within our tissues that is likely to be oxidised and therefore creates greater inflammation. The graph of an approximately 8% finding in 1960 is now up to 23%, a nearly 3 fold increase in the proportion of polyunsaturated fat within the subcutaneous tissue of the body. One would expect the same percentage to be right through every organ in the body.
Oxidation (rust) of the double bond portions of polyunsaturated fat leads to an inflammatory process. The greater the proportion of double bonds in the fat, the higher the rate of oxidation and therefore inflammation.
Saturated fats by definition don’t allow an oxidation pathway to occur.
Monounsaturated fats only really have one double bond which can become oxidised.
Animal fats tend to be predominantly saturated fats and seed oils tend to be mostly polyunsaturated.
It stands to reason that this inflammation appears to be a big contributing factor to our diseased body organs. It certainly creates a susceptible, at risk tissue that is likely to succumb to other processes.
Could this be an explanation of an increased inflammatory process within our bodies and the associated inflammatory conditions in modern disease?
Cardiovascular disease, atherosclerosis
Work has been done to suggest that taking statin drugs can reverse some of the atherosclerotic narrowing within arteries. This is the primary aim of these medications.
It seems a lot simpler to avoid the LDL interaction within the blood vessels in the first place and then prevent inflammation along that line. The statin drugs themselves act as an anti-inflammatory with the blood vessel walls. If you are already on a statin drug then it is reasonable to continue on in consultation with your general practitioner/doctor but there is at least theoretical beneficial effects from cutting down on the fructose and polyunsaturated load to the vessel walls as an adjunct in treatment.
The bonus is that if we are able to reduce that inflammatory load by dietary means, it then has the potential to reduce atherosclerotic disease depending on its degree of advancement. It seems much smarter to address the cause rather than start treating the effects. However, in principle we would much rather take something rather than change something in our lives. This is a hurdle.
Nitric Oxide
Uric Acid has a potent inhibitory effect on Nitric Oxide Synthase which in turns affects Nitric Oxide activity.
There are three main forms of Nitric Oxide Synthase. They all act as Endothelium-Derived Relaxing Factor (EDRF) and have a vasodilatory effect through their action in the production of Nitric Oxide.
eNOS (endothelial Nitric Oxide Synthase)
- Acts on blood vessel endothelium
iNOS (inducible Nitric Oxide Synthase)
- Acts on white cells involved in immunity and tissue damage homeostasis
- Phagocytes
- Neutrophils
- Macrophages
- Monocytes
nNOS (neuronal Nitric Oxide Synthase)
- Acts on the brain and may be involved in the prioritisation of blood and oxygen supply to the brain.
The effect of Uric acid reducing Nitric Oxide bioavailability creates a variety of effects including
- Vasoconstriction and hypertension via its effect on vascular smooth muscle cells
- Oxidative stress in a variety of cells and particularly Adipocytes(fat cells)
- Endothelial cells permeability changes
- ? Immune effect by inhibiting phagocyte (white cell) activity
Another mechanism of tissue damage

ATP is a molecule involved in energy transfer. The phosphate within it is depleted when fructose is metabolised to fructose-1-phosphate by fructokinase. As a result of this depletion of energy stores within tissue, it acts like a form of ischemia with a transient arrest of protein synthesis and further oxidative stress within tissue. It has been associated with the production of inflammatory proteins and the combination of damage within the tissue. Inflammatory proteins may be an issue for the modelling of disease within tissue.
Theoretical Model for Organ Disease and Cancer
The combination of fructose and polyunsaturated oils creates a susceptibility in organ systems and immune-suppression may make us more inclined to develop diseased tissue and cancer.
Cancer Model
There are three phases to the development of a cancer with relationship to my theory. The same applies to most other diseases.
Phase 1
The first is to create low grade inflammation. The cell in an organ then undergoes what is called metaplasia, just like you develop a callus on the bottom of your foot when running barefoot over time. That chronic irritation creates a change in cells. If irritation continues over a longer period of time then those cells can start developing abnormalities and some of them may in fact turn into cancer cells (dysplasia and in to anaplasia).
Phase 2
Those cells then have the ability to divide and if they are in the right inflamed and vascular environment they can potentially grow.
Phase 3
The third aspect is that the body has natural clearing mechanisms within it for taking away abnormal cells and material. There are white cells that are responsible for this activity. Under a Fructose high environment, they appear to have poorer function and motility. This means you have a relatively immunosuppressed system for clearing up any abnormal cells that are developing in the body.
The combination of these three entities with increasing abnormal cells, growing in an inflamed environment and not being able to be cleared away falls well within a model for creating a cancer.
I clearly feel this requires further research and may be that is the next step we are heading to.
The basic tissue damage done by Low Density Lipoproteins (LDL’s) from Fructose metabolism and oxidation from Polyunsaturated Oils is INFLAMMATION in every blood vessel wall and every organ.
Anything that acts as an anti-inflammatory or antioxidant will affect that process.
It makes sense that anti-inflammatories and antioxidants work. It is no wonder that we are constantly made aware of the benefits of drugs or supplements that have these effects. They all theoretically work to some extent. But they cost the Australian economy billions each year.
Aspirin is one of the most widely used anti-inflammatories and has a cardio protective effect.
Statin cholesterol lowering drugs are one of the most prescribed drugs in Australia and have an anti-inflammatory effect.
Niacin (Vitamin B3) has been used for its antioxidant effects.
Non-Steroidal Anti-inflammatories (NSAID’s) are anti-inflammatories readily available now across the counter and used in arthritis and pain management.
Fish oil and Krill oil as omega 3 is sold as an anti-inflammatory.
Vitamin C has antioxidant effects as well as interfering in the Fructose breakdown pathway to Uric Acid.
Tea, berries and a lot of fresh vegetables are touted for their antioxidant effects.
Even moisturiser creams are marketed with their antioxidant effects.
We have two options in this pathway. One is to take a drug in the form of a tablet, drink or supplement. The other is to just cut down on the intake of Sugar and Polyunsaturated Oils and eat more real food. Pretty simple for me.
Oops. That might mean fewer sales for the drug companies and the suppliers of food full of sugar, seed oils and preservatives. It means more sales for the producers of real food.
Please add information by going to Contribute to NoFructose.com
ARTICLES
Metabolic Effects of Fructose and the Worldwide Increase in Obesity
Luc TAPPY and Kim-Anne LE in Physiology Reviews 90: 23–46, 2010; doi:10.1152/physrev.00019.2009.
While virtually absent in our diet a few hundred years ago, fructose has now become a major constituent of our modern diet. Our main sources of fructose are sucrose from beet or cane, high fructose corn syrup, fruits, and honey. Fructose has the same chemical formula as glucose (C6H12O6), but its metabolism differs markedly from that of glucose due to its almost complete hepatic extraction and rapid hepatic conversion into glucose, glycogen, lactate, and fat. Fructose was initially thought to be advisable for patients with diabetes due to its low glycemic index. However, chronically high consumption of fructose in rodents leads to hepatic and extrahepatic insulin resistance, obesity, type 2 diabetes mellitus, and high blood pressure. The evidence is less compelling in humans, but high fructose intake has indeed been shown to cause dyslipidemia and to impair hepatic insulin sensitivity. Hepatic de novo lipogenesis and lipotoxicity, oxidative stress, and hyperuricemia have all been proposed as mechanisms responsible for these adverse metabolic effects of fructose. Although there is compelling evidence that very high fructose intake can have deleterious metabolic effects in humans as in rodents, the role of fructose in the development of the current epidemic of metabolic disorders remains controversial.
Epidemiological studies show growing evidence that consumption of sweetened beverages (containing either sucrose or a mixture of glucose and fructose) is associated with a high energy intake, increased body weight, and the occurrence of metabolic and cardiovascular disorders.
The role of fructose in the pathogenesis of NAFLD and the metabolic syndrome
Nonalcoholic fatty liver disease (NAFLD) is the most frequent liver disease worldwide, and is commonly associated with the metabolic syndrome. Secular trends in the prevalence of these diseases may be associated with the increased fructose consumption observed in the Western diet. NAFLD is characterized by two steps of liver injury: intrahepatic lipid accumulation (hepatic steatosis), and inflammatory progression to nonalcoholic steatohepatitis (NASH) (the ‘two-hit’ theory). In the first ‘hit’, hepatic metabolism of fructose promotes de novo lipogenesis and intrahepatic lipid, inhibition of mitochondrial beta-oxidation of long-chain fatty acids, triglyceride formation and steatosis, hepatic and skeletal muscle insulin resistance, and hyperglycemia. In the second ‘hit’, owing to the molecular instability of its five-membered furanose ring, fructose promotes protein fructosylation and formation of reactive oxygen species (ROS), which require quenching by hepatic antioxidants. Many patients with NASH also have micronutrient deficiencies and do not have enough antioxidant capacity to prevent synthesis of ROS, resulting in necroinflammation. We postulate that excessive dietary fructose consumption may underlie the development of NAFLD and the metabolic syndrome. Furthermore, we postulate that NAFLD and alcoholic fatty liver disease share the same pathogenesis.
‘The Obesity Era’
Facebook blog 25 June 2013
David Berreby looks at some alternative ideas behind obesity ranging from chemicals, to the electrification of society as well as stress. They all may be factors and in my mind are the added stimuli that put our systems over the edge into modern disease states.
I still believe that the combination of Fructose and PUF’s create the inflammation and susceptibility in our organs and these other factors then generate the stimulus for organ failure. Some interesting ideas in the article.
I have taken this quote from well down the article.
‘What are we onlookers — non-activists, non-scientists — to make of these scientific debates? One possible response, of course, is to decide that no obesity policy is possible, because ‘science is undecided’. But this is a moron’s answer: science is never completely decided; it is always in a state of change and self-questioning, and it offers no final answers. There is never a moment in science when all doubts are gone and all questions settled, which is why ‘wait for settled science’ is an argument advanced by industries that want no interference with their status quo.’
http://www.aeonmagazine.com/being-human/david-berreby-obesity-era/
High Levels of Both n-3 and n-6 Long-Chain Polyunsaturated Fatty Acids in Cord Serum Phospholipids Predict Allergy Development by Malin Barman et al in http://www.plosone.org/article/info%3Adoi%2F10.1371%2Fjournal.pone.0067920
Dunder T, Kuikka L, Turtinen J, Räsänen L, Uhari M (2001) Diet, serum fatty acids, and atopic diseases in childhood. Allergy 56: 425–428. doi: 10.1034/j.1398-9995.2001.056005425.x.
Sausenthaler S, Kompauer I, Borte M, Herbarth O, Schaaf B, et al. (2006) Margarine and butter consumption, eczema and allergic sensitization in children. The LISA birth cohort study. Pediatr Allergy Immunol 17: 85–93. doi: 10.1111/j.1399-3038.2005.00366.x.
_________________
The role of macrophage migration inhibitory factor on glucose metabolism and diabetes
More information to follow.