 BASICS
BASICS
- Atherosclerosis
- Hypertension
- Ischaemic heart disease
- Myocardial infarction
- Peripheral vascular disease
- Dementia
The NoFructose Handout Starter Sheet is your take away summary of this web site. Read it at the NoFructose Starter Sheet area of this web site or download it.
IDEAS
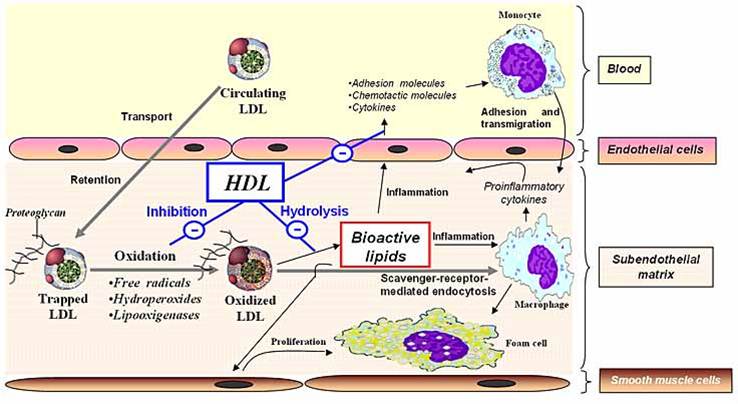
The consumption of Sugar and Polyunsaturated Seed Oils combine in our diet to create inflammation in every blood vessel wall and in every tissue in every organ of the body. The inflammatory process makes everything susceptible to damage and disease.
The inflammation occurs in the subendothelial matrix layer of blood vessel walls as LDL particles become oxidised (rusted).
Read about the Damage Process
Read about the Metabolism
_______________________________
Fructose creates growth of the cardiac muscle that can lead to heart failure.
More evidence for a pathological effect of too much fructose and sugar.
“A new paper by Krek and his team member Peter Mirtschink describes a further, more troubling side effect of fructose. The researchers have discovered a previously unknown molecular mechanism that points to fructose as a key driver of uncontrolled growth of the heart muscle, a condition that can lead to fatal heart failure. Their study was recently published in Nature.
When a person has high blood pressure, the heart has to grow as it is harder to pump the blood through the circulatory system. These growing heart muscle cells require a considerable amount of oxygen. However, since not enough oxygen is available to adequately supply the increased growth, the cells switch to an alternative energy supply. Instead of drawing energy from fatty acids, they rely more on an anaerobic process called glycolysis — literally, the ‘splitting of sugars’. If the heart muscle cells can access fructose in addition to glucose, this can set off a fatal chain reaction.”
http://www.sciencedaily.com/releases/2015/06/150617135038.htm
http://www.nature.com/nature/journal/vaop/ncurrent/full/nature14508.html
_______________________________
Statin Drug Effects
Many patients are on cholesterol lowering statin drugs. They are currently one of the drugs accounting for the majority of drug spending in the western world.
They have an anti-inflammatory effect on the blood vessels and some longitudinal cardiac studies have shown that the blood vessels actually recover to a degree whilst patients are on them. This is effectively a reversal of some of the atherosclerotic inflammatory disease process.
It seems irrational to give anti-inflammatory drugs to a blood vessel when you continue to pour food products on to them creating the same inflammatory process. It is far more effective to avoid the fructose and polyunsaturated oil contributing to the inflammation in the blood vessel walls.
It follows that a reduction of polyunsaturated fats and fructose in the diet will lead to a slowing of the process of atherosclerosis but arguably may actually show a reversal, particularly if there is the added bonus of a reduction in hypertension.
Uric acid, produced as a by-product of fructose metabolism, is a hypertensive agent via its effect of inhibiting nitric oxide on endothelial blood vessel walls.
There is really no down side to cutting out the fructose and polyunsaturated oil in the management of cardiovascular disease, hypertension and its sequelae such as strokes, dementia and renal disease.
However, in principle we would much rather take something rather than change something in our lives. This is a hurdle.
MORE INFORMATION
Hypertension
- Inhibits endothelial Nitric Oxide
- Muscle Insulin Resistance
- Fatty Acid Effect
- Direct effect of uric acid on the adipocyte (fat cell)
- Inflammation and oxidative stress within the adipocyte.
- The effect of fructose consumption causes ATP depletion
- Acts like a type of ischemia
- Transient arrest of protein synthesis
- Production of inflammatory proteins
- Endothelial dysfunction
- Oxidative stress at a tissue level.
ATP is a molecule involved in energy transfer. The phosphate within it is depleted when fructose is metabolised to fructose-1-phosphate by fructokinase. As a result of this depletion of energy stores within tissue, it acts like a form of ischemia with a transient arrest of protein synthesis and further oxidative stress within tissue. It has been associated with the production of inflammatory proteins and the combination of damage within the tissue, inflammatory proteins may be an issue for the modelling of disease within tissue.
Read more about the Damage Process
The NoFructose Handout Starter Sheet is your take away summary of this web site. Read it at the NoFructose Starter Sheet area of this web site or download it.
Please add information by going to Contribute to NoFructose.com

The ongoing stand by recalcitrant bureaucracies to stick to the dictum that ‘saturated fats are bad for your heart’ must end.
http://www.escardio.org/about/documents/eu-cardiovascular-disease-statistics-2012.pdf
21 December 2013
ARTICLES
Added Sugar Intake and Cardiovascular Diseases Mortality Among US Adults.
JAMA Intern Med. 2014 Feb 3. doi: 10.1001/jamainternmed.2013.13563.
Abstract
IMPORTANCE Epidemiologic studies have suggested that higher intake of added sugar is associated with cardiovascular disease (CVD) risk factors. Few prospective studies have examined the association of added sugar intake with CVD mortality. OBJECTIVE To examine time trends of added sugar consumption as percentage of daily calories in the United States and investigate the association of this consumption with CVD mortality. DESIGN, SETTING, AND PARTICIPANTS National Health and Nutrition Examination Survey (NHANES, 1988-1994 [III], 1999-2004, and 2005-2010 [n = 31 147]) for the time trend analysis and NHANES III Linked Mortality cohort (1988-2006 [n = 11 733]), a prospective cohort of a nationally representative sample of US adults for the association study. MAIN OUTCOMES AND MEASURES Cardiovascular disease mortality. RESULTS Among US adults, the adjusted mean percentage of daily calories from added sugar increased from 15.7% (95% CI, 15.0%-16.4%) in 1988-1994 to 16.8% (16.0%-17.7%; P = .02) in 1999-2004 and decreased to 14.9% (14.2%-15.5%; P < .001) in 2005-2010. Most adults consumed 10% or more of calories from added sugar (71.4%) and approximately 10% consumed 25% or more in 2005-2010. During a median follow-up period of 14.6 years, we documented 831 CVD deaths during 163 039 person-years. Age-, sex-, and race/ethnicity-adjusted hazard ratios (HRs) of CVD mortality across quintiles of the percentage of daily calories consumed from added sugar were 1.00 (reference), 1.09 (95% CI, 1.05-1.13), 1.23 (1.12-1.34), 1.49 (1.24-1.78), and 2.43 (1.63-3.62; P < .001), respectively. After additional adjustment for sociodemographic, behavioral, and clinical characteristics, HRs were 1.00 (reference), 1.07 (1.02-1.12), 1.18 (1.06-1.31), 1.38 (1.11-1.70), and 2.03 (1.26-3.27; P = .004), respectively. Adjusted HRs were 1.30 (95% CI, 1.09-1.55) and 2.75 (1.40-5.42; P = .004), respectively, comparing participants who consumed 10.0% to 24.9% or 25.0% or more calories from added sugar with those who consumed less than 10.0% of calories from added sugar. These findings were largely consistent across age group, sex, race/ethnicity (except among non-Hispanic blacks), educational attainment, physical activity, health eating index, and body mass index. CONCLUSIONS AND RELEVANCE Most US adults consume more added sugar than is recommended for a healthy diet. We observed a significant relationship between added sugar consumption and increased risk for CVD mortality.
————-
Linoleic oil poly increases heart disease bmj.e8707.full
Polyunsaturated oil consumption increases cardiovascular events
———————–
Increased egg consumption protects against cardiovascular events
—————————–
The Role of Triglycerides in Atherosclerosis
Current Cardiology Reports. 2011 December ; 13(6): 544–552. doi:10.1007/s11886-011-0220-3
Beatriz G. Talayero, MD, Frank M. Sacks, MD
Summary
Hypertriglyceridemia is a prevalent risk factor for cardiovascular disease (CVD) and increasingly
important in the setting of current obesity and insulin resistance epidemics. High triglyceride (TG)
levels are markers for several types of atherogenic lipoproteins. Patients who have
hypertriglyceridemia may be at significant risk for CVD even if low-density lipoprotein
cholesterol levels are at goal, and therefore warrant treatment that optimizes diet, reduces
overweight, and promotes regular exercise. High-risk patients with hypertriglyceridemia, such as
those with diabetes, CVD, or metabolic syndrome, may benefit from additional drug treatment
aside from a statin to address other lipid abnormalities. In this discussion, we review the role of
hypertriglyceridemia and its associated atherogenic lipoproteins in the pathogenesis of
atherosclerosis, the relevance of a high TG level as a predictor of CVD, the cardiovascular
outcomes from TG-lowering intervention trials, and the current guidelines for treating
hypertriglyceridemia.
Understanding_the_Entire_Lipid_Profile
—————————–
Low Density Lipoproteins Containing Apolipoprotein C-III and the Risk of Coronary Heart Disease
Circulation. 2011 November 8; 124(19): 2065–2072.
doi:10.1161/CIRCULATIONAHA.111.056986.
Carlos O Mendivil, MD, DSc, Eric B. Rimm, DSc, Jeremy Furtado, DSc, Frank M Sacks, MD
Summary
LDL that contains apolipoprotein C-III (apoC-III) comprises only 10 to 20% of plasma LDL, but has a markedly altered metabolism and proatherogenic effects on vascular cells.
Concentrations of LDL with apoC-III (measured as apoB in this fraction) were associated with
risk of CHD in multivariable analysis that included the total cholesterol to HDL cholesterol ratio,
LDL cholesterol, apolipoprotein B, triglycerides, or HDL cholesterol; and other risk factors. In all
models, the relative risks for the top versus bottom quintile of LDL with apoC-III were greater
than those for LDL without apoC-III.
Conclusions—The risk of CHD contributed by LDL appeared to result to a large extent from LDL that contains apoC-III (measured in the Apolipo B number)
———————————————–
Acute Effect of Cigarette Smoking on Glucose Tolerance and Other Cardiovascular Risk Factors
Alberto C Frati, MD, FACP, Felipe Iniestra, MD and C Raul Ariza, MD, FACP
doi: 10.2337/diacare.19.2.112 Diabetes Care February 1996 vol. 19 no. 2 112-118
CONCLUSIONS Smoking acutely impaired glucose tolerance and insulin sensitivity, enhanced serum cholesterol and triglyceride levels, and raised blood pressure and heart rate. These findings support the pathogenetic role of cigarette smoking on cardiovascular risk factors.
——————————————–
Blood glucose and risk of cardiovascular disease in the Asia Pacific region.
Diabetes Care. 2004 Dec;27(12):2836-42.
Abstract
OBJECTIVE:
To assess the shape and strength of the association between usual blood glucose and cardiovascular disease (CVD) in Asian and Australasian cohorts and to determine the impact of adjusting for other determinants of CVD risk and excluding people with diabetes.
RESEARCH DESIGN AND METHODS:
Relative risk estimates and 95% CIs were calculated from Cox models, stratified by sex and cohort, and adjusted for age at risk on individual participant data from 17 cohort studies. Repeat measurements of blood glucose were used to adjust for regression dilution bias.
RESULTS:
Fasting blood glucose data were available for 237,468 participants, and during approximately 1.2 million person-years of follow-up, there were 1,661 stroke and 816 ischemic heart disease (IHD) events. Data were also available on 27,996 participants with nonfasting glucose measurements. Continuous positive associations were demonstrated between usual fasting glucose and the risks of CVD down to at least 4.9 mmol/l. Overall, each 1 mmol/l lower usual fasting glucose was associated with a 21% (95% CI 18-24%) lower risk of total stroke and a 23% (19-27%) lower risk of total IHD. The associations were similar in men and women, across age-groups, and in Asian compared with Australasian (Australia and New Zealand) populations. Adjusting for potential confounders or removing those with diabetes as baseline did not substantially affect the associations. Associations for nonfasting glucose were weaker than those with fasting glucose.
CONCLUSIONS:
Fasting blood glucose is an important determinant of CVD burden, with considerable potential benefit of usual blood glucose lowering down to levels of at least 4.9 mmol/l.
______________________________
New insights into the health effects of dietary saturated and omega-6 and omega-3 polyunsaturated fatty acids
2012
 1 and
1 and Cardiovascular diseases and cancers are leading causes of morbidity and mortality. Reducing dietary saturated fat and replacing it with polyunsaturated fat is still the main dietary strategy to prevent cardiovascular diseases, although major flaws have been reported in the analyses supporting this approach. Recent studies introducing the concept of myocardial preconditioning have opened new avenues to understand the complex interplay between the various lipids and the risk of cardiovascular diseases. The optimal dietary fat profile includes a low intake of both saturated and omega-6 fatty acids and a moderate intake of omega-3 fatty acids. This profile is quite similar to the Mediterranean diet. On the other hand, recent studies have found a positive association between omega-6 and breast cancer risk. In contrast, omega-3 fatty acids do have anticancer properties. It has been shown that certain (Mediterranean) polyphenols significantly increase the endogenous synthesis of omega-3 whereas high intake of omega-6 decreases it. Finally, epidemiological studies suggest that a high omega-3 to omega-6 ratio may be the optimal strategy to decrease breast cancer risk. Thus, the present high intake of omega-6 in many countries is definitely not the optimal strategy to prevent cardiovascular disease and cancers. A moderate intake of plant and marine omega-3 in the context of the traditional Mediterranean diet (low in saturated and omega-6 fatty acids but high in plant monounsaturated fat) appears to be the best approach to reduce the risk of both cardiovascular diseases and cancers, in particular breast cancer.
More to follow